Physical Therapists' Role in Screening for Eating Disorders by Autumn Harless
Statistics have shown that Anorexia Nervosa (AN) has the highest mortality rate of all mental disorders and around 24 million people in the United States are struggling with an eating disorder. 1, 2 Eating disorders are a challenging and debilitating diagnoses due to its complexity, difficulty diagnosing, multiple factors, and lack of awareness and attention. Due to the COVID-19 pandemic, there has been a rise in the number of eating disorder diagnoses and many people struggling have reported an increase in their symptoms due higher levels of stress and anxiety. 1 With this spike in numbers, it is vital that eating disorders are not only diagnosed but found early to allow for proper treatment and prevent negative consequences and adverse effects that come along. This currently involves an interprofessional team of medical providers, however, there is limited evidence of the involvement of physical therapists.
The American Psychiatric Association defines an eating disorder as, “behavioral conditions characterized by severe and persistent disturbance in eating behaviors and associated with distressing thoughts and emotions.” 3 The Diagnostic and Statistical Manual of Mental Disorders contains information on classifications of eating disorders, screening and diagnostic tools, and treatments. This was updated in 2013 to the fifth edition where classifications of eating disorders were reconditioned and thoroughly defined. 4 If physical therapists want to play an active role in the screening of eating disorders, it is important to understand the different classifications and common characteristics seen within those to help with the screening process.
The first category of eating disorder and one of the most prevalent and leading mortality rates is Anorexia Nervosa (AN). 2 The DSM refers to Anorexia Nervosa as a decrease in caloric and energy intake with a decreased body mass index (BMI) that is appropriate for the person's age, gender, etc. Usually people with anorexia have increased fear of weight gain and have the perception that they are “fat” or “overweight”. 4 The second most common eating disorder is Bulimia Nervosa (BM). This is classified as a period of eating followed by an unhealthy habit: such as self induced vomiting; use of laxatives, diuretics, and other medications; or periods of fasting or increased exercise. 4 Both of these diagnoses are heavily influenced by self image and therefore are common in athletes, especially females but can occur in males or other populations as well. 3 This is a population that many physical therapists will come into contact with whether in an outpatient orthopedic or sports specialty.
Another important category of eating disorders is Binge Eating Disorder (BED) which is similar to Bulimia Nervosa, however, is not followed by compensatory actions. Binge Eating is commonly referred to as heavy periods of eating with a feeling of “lack of control” or “no ability to stop.” This results in negative thoughts or feelings post binge due to the amount of food intake. 4 Next is Avoidant/Restrictive Food Intake Disorder (ARFID) which consists of a decreased food intake causing an effect on nutritional needs for proper health and development. 4 Pica is another type of eating disorder which is when a person eats items that are not considered food and does not provide any nutritional benefit. This is a normal part of development and environmental exploration in children so this cannot be diagnosed under the age of two. Pica is often seen in Autism Spectrum Disorder (ASD), therefore, pediatric physical therapists could have an important role with this category because they are often working with this population or an age range where Pica is likely seen. 4 Lastly is Other Specified Feeding or Eating Disorder (OSFD) which includes characteristics of eating disorders but does not meet full criteria of any of the above mentioned diagnoses. 4
Even though signs can be visible at times regarding eating disorders, it is still important to use screening tools in order to determine a need for referral or treatment. Medical providers use a variety of screening tools. Physicians depend on screening and getting some information during a subjective examination including: determining any factors that put the patient more at risk for eating disorders; any signs and symptoms mentioned earlier in the DSM fifth edition criteria; and any personal or family history with eating disorders, anxiety, or depression. 5 The American Psychiatric Association created a Clinical Practice Guideline that also focuses on the screening process where they dig into history of weight over the years; any patterns in eating, exercising, or other compensatory behaviors (as mentioned in Binge Eating); and any other psychological conditions. 6
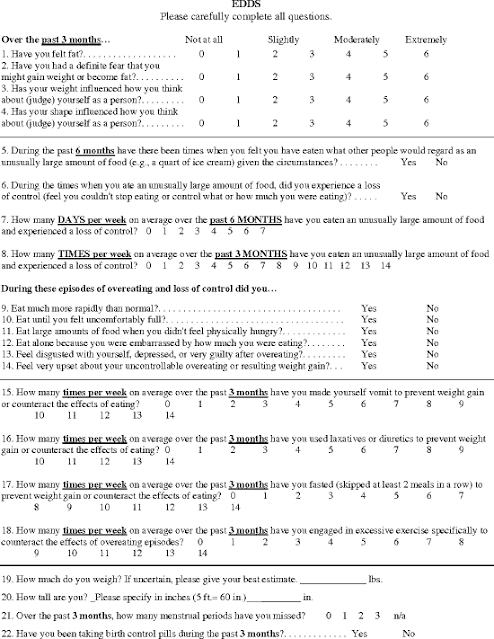
Questionnaires are also often used throughout multiple professions such as physician, psychiatrist, dietician, and nutritionist as a screening tool for eating disorders. The Eating Disorder Diagnostic Scale (EDDS) is a common tool and is a 22-item questionnaire that can be utilized to determine if an eating disorder is suspected and which DSM IV edition category it is most likely. There is now an updated EDDS which contains 23 questions and uses the DSM V edition, however, psychometrics data is not out yet on this update. Many medical providers utilize this tool because it is a quick yet through screening tool to help determine at risk patients for eating disorders. 7, 8
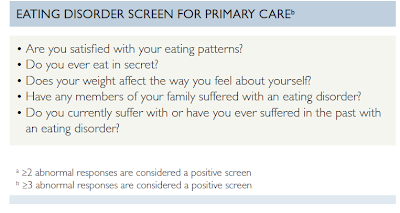
The National Eating Disorder Collaboration has multiple recommendations for screening. One of the most used is the Eating Disorder Screen for Primary Care (ESP). This is an extremely quick 5-item questionnaire to help to determine if an eating disorder is suspected and a referral is needed. This tool uses a cutoff of 2 or more abnormal responses and has a 100% sensitivity and 71% specificity. Therefore, it an extremely beneficial screen if there is a suspicion of an eating disorder which makes it the tool of choice often.9, 10
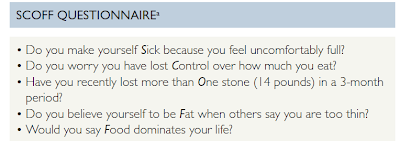
Another useful screening tool that the National Eating Disorder Collaboration and other sources recommend is the SCOFF. The SCOOF is an effective acronym screen used by medical providers to rule in the chance of eating disorders. This tool also has a cutoff of 2 or more abnormal responses. This tool has a 78% sensitivity and 88% specificity. 9, 10 The Eating Disorder Examination-Questionnaire (EDE-Q) is a more extensive screening tool that focuses on different areas of concern. The screen consists of 28 questions with specific “dietary restraints, eating concerns, weight concerns, and shape concerns.” 9, 11
Current studies state that the multidisciplinary team approach is the most beneficial and effective approach in regards to eating disorders. Currently, “Team members include a physician, a nutritionist, and a mental health professional.” 5, 12 Does a physical therapist fit within this scope? Can they play an integrative part on the team and help with the screening process in order to help patients get the referrals needed to start their recovery process? The American Psychiatric Association states “Because primary care professionals are likely to be the first clinicians who encounter patients with eating disorders, it is important for them to be able to effectively and efficiently diagnose these patients and make appropriate referrals. 13
As mentioned previously, female athletes are at higher risk for eating disorders and pica is also oftentimes seen in children with Autism Spectrum Disorder. These are two populations that physical therapists frequently work with and treat. Outpatient orthopedic clinics and sports specialty clinics have a high volume of athletes and would benefit from having screening tools on hand to take every athlete through to ensure the safety and health of every athlete. Pediatric physical therapists work often with children with ASD. They also focus on developmental stages and have the potential to catch symptoms of eating disorders early on. Additionally, physical therapists can be direct access and PT’s spend increased quantities of time with patients which gives more opportunities to pick up on any signs and symptoms or eating disorders. Physical therapists also create special bonds with their patients by creating a welcoming and trusting environment. Therefore, overtime patients many times open up regarding their thoughts and feelings.
With the increased prevalence of eating disorders, this is an issue that needs to be addressed and have more awareness around. Many eating disorders go unknown and unrecognized, and physical therapists have a special talent of connecting with their patients and have the potential to catch those who need help. There is a current multidisciplinary team to address these diagnoses, however, physical therapists could also play a vital role in helping with the screening process in order to get patients the proper referrals and treatment they need.
References
Reed J, Ort K. The Rise of Eating Disorders During COVID-19 and the Impact on Treatment. J Am Acad Child Adolesc Psychiatry. 2022;61(3):349-350. doi:10.1016/j.jaac.2021.10.022
Chesney E, Goodwin GM, Fazel S. Risks of all-cause and suicide mortality in mental disorders: a meta-review. World Psychiatry. 2014;13(2):153-160. doi:10.1002/wps.20128
Guarda A. Eating disorders. Psychiatry.org - Eating Disorders. Accessed November 18, 2023. https://www.psychiatry.org/patients-families/eating-disorders.
American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders. 5th ed. Washington D.C.: 2013.
Walsh JM, Wheat ME, Freund K. Detection, evaluation, and treatment of eating disorders the role of the primary care physician. J Gen Intern Med. 2000;15(8):577-590. doi:10.1046/j.1525-1497.2000.02439.x
American Psychiatric Association publishes updated guideline on Eating disorders and accompanying Im. Psychiatry.org - American Psychiatric Association Publishes Updated Guideline on Eating Disorders and Accompanying Im. February 27, 2023. Accessed November 18, 2023. https://www.psychiatry.org/news-room/news-releases/apa-updated-guideline-on-eating-disorders.
Admin A. Eating disorder diagnostic scale (EDDS). PsychTools. March 9, 2018. Accessed November 18, 2023. https://www.psychtools.info/edds/.
Krabbenborg MA, Danner UN, Larsen JK, et al. The Eating Disorder Diagnostic Scale: psychometric features within a clinical population and a cut-off point to differentiate clinical patients from healthy controls. Eur Eat Disord Rev. 2012;20(4):315-320. doi:10.1002/erv.1144
Screening and assessment tools for eating disorders - NEDC. Screening and Assessment for Eating Disorders. Accessed November 18, 2023. https://nedc.com.au/assets/PHN/Fact-sheets/Screening-and-assessment-tools-for-eating-disorders.pdf.
Cotton MA, Ball C, Robinson P. Four simple questions can help screen for eating disorders. J Gen Intern Med. 2003;18(1):53-56. doi:10.1046/j.1525-1497.2003.20374.x
Schaefer LM, Crosby RD, Machado PPP. A systematic review of instruments for the assessment of eating disorders among adults. Curr Opin Psychiatry. 2021 Nov 1;34(6):543-562. doi: 10.1097/YCO.0000000000000746. PMID: 34475351; PMCID: PMC8645259.
Joy EA, Wilson C, Varechok S. The multidisciplinary team approach to the outpatient treatment of disordered eating. Curr Sports Med Rep. 2003;2(6):331-336. doi:10.1249/00149619-200312000-00009
The American Psychiatric Association launches new eating disorder clinical decision support tool. Psychiatry.org - The American Psychiatric Association Launches New Eating Disorder Clinical Decision Support Tool. May 23, 2023. https://www.psychiatry.org/news-room/news-releases/apa-launches-new-eating-disorders-decision-tool.

